
Updated August 28, 2024
NCCID Disease Debriefs provide Canadian public health practitioners and clinicians with up-to-date reviews of essential information on prominent infectious diseases for Canadian public health practice. While not a formal literature review, information is gathered from key sources including the Public Health Agency of Canada (PHAC), the USA Centers for Disease Control and Prevention (CDC), the World Health Organization (WHO) and peer-reviewed literature.
This disease debrief was prepared by Heather Long and Wendy Xie. Questions, comments, and suggestions regarding this disease brief are most welcome and can be sent to nccid@manitoba.ca
What are Disease Debriefs? To find out more about how information is collected, see our page dedicated to the Disease Debriefs.
Questions Addressed in this debrief:
- What are important characteristics of the mpox virus?
- What is happening with current outbreaks of mpox?
- What is the current risk for Canadians from mpox?
- What measures should be taken for a suspected mpox case or contact?
What are important characteristics of the mpox virus?
Cause
mpox virus (formerly Monkeypox) is a double-stranded DNA virus belonging to the Orthopoxvirus genus in the family Poxviridae, which includes human variola (VAR), cowpox (CPV), and vaccinia (VAC) viruses. mpox virus is a zoonotic disease, meaning it can be transmitted from animals to humans. Squirrels, Gambian pouched rats, dormice, and non-human primates have been found to be susceptible to mpox virus, but further research is required to identify the true natural reservoir(s). There are two genetic clades of the mpox virus – the Central African (Congo Basin) and West African clades. The Congo Basin clade has caused more severe disease and is thought to be more transmissible.
mpox virus transmission occurs when a person comes into direct or indirect contact with the body fluids or lesion materials of infected animals and humans, including contaminated materials. Animal-to-human transmission may occur by bite or scratch, or through the preparation of bush meat. Human-to-human transmission of mpox virus is thought to occur primarily through respiratory droplets during sustained face-to-face contact, but may also be sexually transmitted through contact with the body fluids of an infected person. The virus may enter the body through broken skin (even if not visible), the respiratory tract, or mucous membranes of the eyes, nose, or mouth.
Signs and Symptoms, and Severity
The symptoms of mpox virus are milder than, but similar to those of smallpox. One key difference is that mpox causes swollen lymph nodes (lymphadenopathy) while smallpox does not. The swelling can occur in many different locations on the body, or be localized, including lymph nodes of the neck and armpit. The incubation period (time from infection to onset of symptoms) for mpox is usually 7−14 days but can range from 5−21 days. In addition to swollen lymph nodes, early signs and symptoms may include fever, headache, muscle aches, exhaustion, backache, and chills. A rash develops on the body within 1 to 3 days (sometimes longer) after the appearance of fever, usually first on the face, then spreading to other parts of the body. The lesions progress through the stages of macules, papules, vesicles, pustules, and finally scabs before falling off.
At the Meeting of the International Health Regulations Emergency Committee held on June 23, 2022, it was noted that the clinical presentation in the current mpox outbreak is often atypical. There are fewer lesions observed, and the lesions are often localized to the genital, perineal/perianal or peri-oral area. Some cases involve an asynchronous rash appearing prior to the prodromal phase (lymphadenopathy, fever, malaise). On April 28th, 2023, the WHO published the Atlas of mpox lesions, which is a compilation of mpox lesion images to show examples of the infection in the skin and mucosa to be used as a tool for clinical researchers.
On August 25, 2022, the WHO released an updated interim guidance on surveillance stating that patients are presenting with more mucosal lesions than previously reported. These mucosal lesions are often localized in the genital and anal regions as well as in the mouth and on the eyes. It has also been noted that the rash can develop prior to the usual symptoms such as fever and fatigue. Anal pain and bleeding and swollen lymph nodes remain common.

Illness can last for 2-4 weeks depending on the health of the infected individual, the clade of the infecting virus, and the route of exposure. The disease has been shown to cause death in 0-11% of documented cases, with higher mortality rate observed in young children. Pregnant or breastfeeding women, children, persons with underlying medical conditions or immunocompromised individuals may be at higher risk for severe illness due to mpox infection. Among mpox patients in the US, the majority of people with severe manifestations of mpox infection were substantially immunocompromised as a result of human immunodeficiency virus (HIV) infection. The CDC recommends that healthcare providers be aware of immunocompromising conditions (including HIV) and medications which can contribute to severe mpox infections. Healthcare providers should conduct HIV testing for people with confirmed or suspected mpox infection. For additional information on severe manifestations of mpox infection, see here.
PHAC: Public Health News – mpox
WHO: Multi-country mpox outbreak in non-endemic countries
WHO: Meeting of International Health Regulations Emergency Committee (June 25, 2022)
WHO: Interim Guidance on Surveillance (Aug 25, 2022)
WHO: Atlas of mpox lesions (April 28, 2023)
CDC: mpox – Clinical Recognition
CDC: Guidance for Tecovirimat Use
Epidemiology
Since the discovery of mpox virus in 1958, infections have been reported in people in central and western African countries: Cameroon, Central African Republic, Côte d’Ivoire, Democratic Republic of the Congo, Gabon, Liberia, Nigeria, Republic of the Congo, and Sierra Leone, with most infections occurring in the Democratic Republic of the Congo. Outside of Africa, most mpox cases in humans have been linked to international travel or exposure to imported animals, including cases in the United States, Israel, Singapore, and the United Kingdom. Many recently reported cases of mpox from Sweden, Italy, Belgium, USA and Canada are not linked to travel to the endemic areas of West/Central Africa, suggesting that there is local transmission within communities. In the UK, Spain and Portugal, cases of mpox have been reported amongst, but not exclusively in, men who have sex with men (MSM).
According to the World Health Organization (WHO), there were a total of 102,997 laboratory-confirmed cases of mpox including 223 deaths reported from 121 countries from January 1, 2022 through July 31, 2024. As of July 2024, WHO reports that the number of monthly reported new cases has increased by 8.8% compared to the previous month, with the majority of cases being reported from the African Region (54.9%) and the Region of the Americas (24.2%). Since January 1, 2022, the 10 most affected countries globally are the United States of America (n = 33 556), Brazil (n = 11 841), Spain (n = 8 104), Democratic Republic of the Congo (n = 4 385), France (n = 4 283), Colombia (n = 4 256), Mexico (n = 4 132), The United Kingdom (n = 4 018), Peru (n = 3 939), and Germany (n = 3 886). Together, these countries account for 80.0% of the cases reported globally. In the past six months, the most affected region was the African Region, where 3061 cases and 23 deaths have been reported. Clades Ia, Ib, and II have been reported in the African Region.
As of July 31, 2024, 96.4% of cases were reported in men (median age 34 years), with males between 18-44 years old disproportionately affected by this outbreak (79.3% of reported cases). In the available data, 3.6% of cases were reported to be in women, of which the majority were reported from the Region of the Americas (74%) and the European Region (14%). Global trends of the mpox outbreak can be found on the WHO 2022-2024 dashboard (produced on August 22, 2024).
Of cases with HIV status information available, 51.9% (18,628 of 35,861 cases) of cases are reported to be in persons living with HIV and is related to the common risk factor of sexual exposure between the two conditions. As information for HIV status is not available for most cases in the WHO African Region, the above description may not be fully representative of cases in this region.
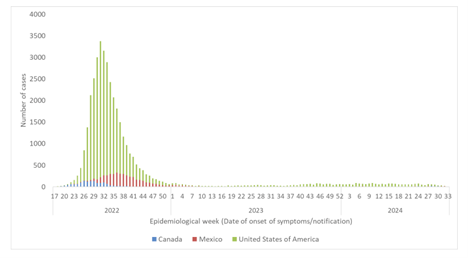
In an update published on August 17, 2024, the Pan American Health Organization (PHAO) reported that between 2022 up to August 17, 2024, there have been 39,149 cases of mpox reported in the North American subregion (Canada, Mexico, United States of America), including 94 deaths (Figure 1). The United States of America reported 85% of cases in the North American subregion. In July 2024, the WHO reported that the United States of America had a 0.5% increase in cases compared to June 2024 (200 cases compared to 199 cases), Canada reported a 39.0% decrease in monthly cases (14 cases in July 2024 compared to 23 cases in June 2024), Mexico reported a 36.0% decrease in monthly cases (7 cases in July 2024 compared to 11 cases in June 2024).
Figure 1. Confirmed cases of mpox by epidemiological week of onset of symptoms/notifications and country in the subregion of North America (Canada, Mexico, and the United States of America) as of August 17, 2024.
The Public Health Agency of Canada (PHAC) published an Epidemiological summary report detailing the mpox outbreak in Canada from 2022 to 2023. Between May 19, 2022 and December 31, 2023, a total of 1541 mpox cases were reported to PHAC, with 1465 confirmed cases and 76 probable cases. Most reported cases were locally acquired in Canada, with only 8% reporting international travel in the 3 weeks prior to symptom onset. Of all cases reported to PHAC between May 2022 and December 2023, 96% were reported in Ontario, Quebec, and British Columbia. As of December 31, 2023, 272 sequences representing at least 162 unique confirmed mpox cases in Canada (11% of total confirmed cases to this date) were assembled and established as Clade IIb by PHAC’s National Microbiology Laboratory (NML). Among cases reported between May 19, 2022 and December 31, 2023, 97.7% of confirmed and probable mpox cases were reported in men (1,349 of 1,381 total cases). Of all confirmed and probable mpox cases during this period, the highest proportion of reported cases (39.9%) were within the 30-39 years age group. These results may not be representative of cases reported in Canada after December 31, 2023.
PHAC: Epidemiological summary report: 2022-2023 mpox outbreak in Canada (June, 2024)
WHO: 2022-24 Mpox Outbreak: Global Trends (August 22, 2024)
CDC: mpox in the United States
PAHO: Epidemiological Update Mpox in the Americas Region (August 17, 2024)
Laboratory Diagnosis
A confirmed diagnosis of a mpox infection requires one or more of the following diagnostic markers to be positive:
- Presence of mpox virus DNA detected using polymerase chain reaction (PCR).
- Isolation of mpox virus from viral culture.
The best specimens for PCR and isolation are skin lesion material, including swabs of lesion surface or fluid, crusts/scabs, and roofs of multiple lesions. Lesion material should be transported in an empty, sterile container.
Serology is not the preferred method due to cross-reactivity with previously smallpox vaccinated individuals and other Orthopoxviruses. Given the ongoing multi-country outbreak, the Public Health Agency of Canada (PHAC) National Microbiology Lab (NML) is relaxing the requirement to demonstrate travel to mpox virus endemic areas or contact to travellers or animals from these areas.
PHAC: For Health Professionals – Diagnosis (June 4, 2024)
Prevention and Control
On May 24, 2024, the World Health Organization (WHO) announced the strategic framework for enhancing infection prevention and control of mpox for 2024 to 2027. This framework outlines a roadmap for health authorities, communities and stakeholders globally to control mpox outbreak, minimize zoonotic transmission, advance mpox research and access to counter measures. The framework calls for international cooperation, resource sharing, and stakeholder support at local, national, and global levels to address existing inequities and advance broader pandemic preparedness through strengthened capacities in collaborative surveillance and response.
The Public Health Agency of Canada (PHAC) provided Interim Guidance on infection prevention and control for suspect, probable or confirmed mpox within Healthcare settings, dated May 27, 2022 advisesany lesions or respiratory secretions should be considered infectious material. Routine practices should include:
- Point of Care Risk Assessment (PCRA)
- Hand Hygiene (alcohol-based hand sanitizers and soap, washing hands after removing gloves)
- Patient Placement
- Respiratory hygiene
- Personal Protective Equipment (PPE)
- Injection and Medication Safety
- Cleaning and Disinfection Procedures
- Waste Management
Airborne, droplet, and contact precautions are recommended as follows:
Patient:
- Wash hands
- Wear a medical mask
- Upon entry to a healthcare setting, suspect, probable and confirmed cases should be immediately placed into an Airborne Infection Isolation Room (AIIR) or single room with the door closed.
- If clinically tolerable, patient must wear a medical mask when leaving the room.
- Cover skin lesions with a gown, clothes, sheet or bandage, except during examination.
- Disinfect room after use
Health care worker – Personal Protective Equipment (PPE):
- N95 respirator
- Cuffed, long sleeve gown
- Gloves
- Eye protection
Discard all PPE including respirators after contact with the patient. Perform hand hygiene. Wear all PPE entering the patient’s room and dispose of all PPE prior to leaving the isolation room except for the respirator. Remove respirator outside of the room once the door is closed. Perform hand hygiene again.
Room Selection/Patient Placement:
Place patient in an AIIR, when available or place patient in a single room with the door closed. Inpatients should have their own bathroom or a commode can be used if a dedicated bathroom is not available.
Restrict visitors to those necessary for care or compassionate grounds.
Cleaning and Disinfection:
- Standard disinfection protocols.
- Dedicate patient care equipment to a single patient.
- Disinfect all reusable equipment with hospital-approved disinfectants immediately after use.
Environmental surfaces:
Disinfect all contact surfaces with hospital-approved disinfectants including chairs, doorknobs, call bell pulls, faucet handles, wall surfaces and public bathrooms. Use standard housekeeping cleaning and disinfection protocols.
Laundry (such as linens, towels, clothing, bedding):
- Wear appropriate PPE (gloves, gown, fit-tested and seal-checked N95 respirator and eye protection) during collection and bagging of all linens.
- Laundry should be transferred to a sealed and tied into a leak-proof bag and placed inside an impermeable bag for transport to laundry area.
- In ambulatory care settings, standard medical laundry facilities should be used however it not available, laundry may be washed in a standard washing machine using hot water (70 degrees Celsius) with detergent and must be completely dried in a commercial dryer.
- avoid contact with the worker’s skin and clothing when handling soiled laundry (clothing, towels, bedding)
- Do not shake laundry, as it disperses contaminated infectious particles into the air and onto the surrounding surfaces.
Containment and Disposal of Contaminated Waste:
- Biomedical waste should be contained in impervious waste-holding bags or double bagged.
- Contaminated disposable items should be discarded according to jurisdictional protocols.
Discharge environmental cleaning and disinfection:
- HCW must wear a gown, gloves, fit-tested and seal-checked N95 respirator and eye protection during cleaning and disinfection as per disinfection protocols.
- Discard all disposable items in patient’s room.
- Change privacy curtains.
- Discard any equipment/supplies that cannot be disinfected.
Transportation of suspected mpox patients:
Patient should not use public transportation and should wear a mask and cover all lesions during transport. Patient transport services should be informed that the patient has suspect, probable, or confirmed mpox beforehand and the receiving healthcare setting should be informed of the need for airborne, droplet and contact precautions.
According to the World Health Organization an exposed health care worker who is asymptomatic does not need to isolate and can remain on the job, however will need to actively monitor themselves for 21 days, monitoring one’s temperature twice per day and should have an interview with their local occupational health office before returning to work. If the health care worker becomes symptomatic, they should not return to work and will need to isolate at home until they are no longer considered contagious, when all symptoms have subsided and all scabs are completed healed over. This can take between 2 to 4 weeks.
PHAC: Prevention and Control (posted June 1, 2022)
WHO: Exposed Healthcare Provider Guidance
WHO: Strategic framework for enhancing prevention and control of mpox 2024-2027 (May 24, 2024)
Treatment and Vaccination
Most cases of mpox infection are self-limiting and symptoms will resolve on their own if rashes are left to dry or covered with a moist dressing to protect the area. There is currently no proven and safe treatment for mpox virus infection, however, vaccinia immune globulin (VIG) and antivirals may be recommended for severe cases. Tecovirimat (or TPOXX) is an antiviral that was developed to treat smallpox and has also been approved for the treatment of mpox in January 2022. Relevant adverse events related to TPOXX can be directly reported to the Canada Vigilance Program through the Health Canada website. Other antivirals including Cidofovir and Brincidofovir are all currently being tested for activity against mpox virus.
Imvamune is a 3rd generation smallpox vaccine licensed for active immunization against smallpox, mpox , and related Orthopoxvirus infection and disease in adults 18 years and older with high risk for exposure. Provincial and territorial public health authorities have started vaccinating populations at higher risk. To date, human-to-human spread of mpox can be controlled via early diagnosis and treatment of symptoms, isolation of patient and contact tracing. For individuals who are contacts of cases, post-exposure prophylaxis (PEP) with a second- or third-generation vaccine is recommended. To prevent the onset of disease, this vaccine should be provided within four days of first exposure and up to 14 days in the absence of symptoms. The Interim guidance on the use of Imvamune in the context of a routine immunization program (National Advisory Committee on Immunization) published on May 24, 2024 recommends that individuals at high risk of mpox should receive two doses of Imvamune administered at least 28 days (4 weeks) apart.
For health care workers and laboratory staff at high risk of exposure to mpox cases, pre-exposure prophylaxis (PrEP) is recommended.
On August 12, 2022, PHAC released a Statement from the Chief Public Health Officer of Canada which stated that to date, the Government of Canada has deployed over 99,000 doses of Imvamune vaccine to provinces and territories and is working to secure future supplies of both vaccines and therapeutics while providing treatment for case management. As of August 11, 2022 , over 50,000 Canadians have now been vaccinated.
In cases of severe manifestations of mpox infection in immunocompromised patients (due to HIV or other immunocompromising conditions), the Centers for Disease Control and Prevention (CDC) recommends that mpox treatment should include limiting the use of immunosuppressive medications unless otherwise clinically indicated. For mpox patients with HIV, providing retroviral therapy is recommended. To treat severe illness due to mpox infection, oral and intravenous tecovirimat (TPOXX), cidofovir or brincidofovir, and vaccinia immune globulin intravenous (VIGIV) may be used, but data on the effectiveness of these countermeasures in treating human mpox is still lacking. For more recommendations for healthcare providers on treatment of mpox infection in immunocompromised patients, see here.
PHAC: Statement from Chief Public Health Officer (August 12, 2022)
PHAC: Summary of NACI Interim Guidance (June 10, 2022)
PHAC: Update on Imvamune Vaccination (June 27, 2022)
PHAC: Management and treatment (July 15, 2022)
PHAC: Update on mpox in Canada (July 27, 2022)
Health Canada: Report a side effect of a health product, drug, or medical device
NACI: Interim Guidance on the use of Imvamune in the context of mpox in Canada (June 2022)
CDC: Guidance for Tecovirimat Use
What is happening with current outbreaks of mpox ?
According to the World Health Organization a total of 934 new laboratory confirmed cases of mpox and four deaths have been reported in 26 countries in June 2024. The most affected regions include the WHO African region, the European Region, the Regions of the Americas, the Western Pacific Region, and the South-East Asian Region.
Since 2023, the emergence and rapid spread of a new virus strain Clade 1b mpox in the Democratic Republic of Congo (DRC). So far, about 19,919 Clade 1 mpox cases have been reported in 2023 and 2024, with 975 (4.9%) mortalities. A large proportion of the current outbreak is among children age 15 and under (67% suspected cases and 78% suspected deaths).
In a recent news release on August 12, 2024, the Director General of the World Health Organization (WHO) declared the upsurge of mpox in the Democratic Republic of the Congo (DRC) and a growing number of countries to be a public health emergency of international concern (PHEIC). The Director General had previously triggered the process for Emergency Use Listing for mpox vaccines to accelerate vaccine access for lower-income countries which have not yet issued a national regulatory approval. The WHO is working with countries, vaccine manufacturers, and partners to facilitate equitable access to vaccines, therapeutics, diagnostics, and other tools.
The Public Health Agency of Canada (PHAC) provides an outbreak update of mpox cases across provinces and territories in Canada up to September 29, 2023. The Centers for Disease Control and Prevention (CDC) provides a summary of the confirmed cases in the United States and worldwide.
WHO: Press Conference (July 23, 2022)
WHO: Multi-country outbreak of mpox – 35th situation report (August 12, 2024)
CDC: Global mpox Outbreak Update
What is the current risk for Canadians?
As of July 23, 2022, the World Health Organization (WHO) maintains the risk to be moderate at the global level, apart from the European region, where the risk is high. The WHO recommends that all countries work closely with the men who have sex with men (MSM) community and HIV patients to communicate information and services available to protect the health of those affected and fight against stigma. The Director of the WHO has made recommendations for regions based on their current epidemiological situation, patterns of transmission and capacities, which can be found here.
On August 12, 2022, the Centre for Disease Control stated that although it is still not known whether those living with HIV are at an increased risk to acquire mpox , those with advanced HIV might be at a higher risk for severe mpox . They emphasize the importance of prompt diagnosis and treatment in this population and are recommending postexposure prophylaxis and antiviral treatments for those living with HIV.
There is added risk to health workers if they are not using adequate infection prevention and control (IPC) measures or wearing appropriate personal protective equipment (PPE) to reduce the risk of transmission. In Canada, cases of human transmission have involved close contact with an infected individual, but the risk to the general public remains low. However, this is an ongoing investigation in Canada and around the world, and more information is needed to determine the risk to Canadians. The Public Health Agency of Canada (PHAC) will continue to release recommendations to minimize the risk of infection and provide updates related to confirmed cases. Given that the vvirus is spread through close contacts, PHAC advises physical distancing, handwashing, and wearing masks to reduce the risk of infection. While the risk of infection for the general population is low, PHAC recommends that Canadians and health care providers should be aware of the symptoms of mpox regardless of travel history. PHAC also recommends that using condoms, practicing safe sex, and having fewer sexual partners (anonymous partners in particular) even when they do not have symptoms can also reduce the risk of becoming infected with mpox .
The Centers for Disease Control and Prevention (CDC) does not see any evidence to date that mpox poses a high risk to domestic pets. In a past outbreak in the United States in 2003, there was no evidence to suggest the disease was spread from humans to their domestic pets. Regardless, the CDC recommends anyone with mpox to avoid contact with their pets and make arrangements for someone to care for their pets until they recover.
Until more is known about which mammals are susceptible to infection it is best to assume that any mammal can be infected with mpox . For the most recent information about mpox in animals please refer to the Centre for Disease Control’s update here.
PHAC: Update on mpox in Canada (July 23, 2022)
WHO: Multi-country mpox outbreak update (June 4, 2022)
WHO: Press Conference (July 23, 2022)
WHO: International Health Regulations 2nd Emergency Meeting (July 23, 2022)
CDC: mpox in HIV population (August 12, 2022)
CDC: mpox in Animals (August 12, 2022)
Travel Advisory
Canadians traveling abroad may now register with the Government of Canada here to access the latest information in the case of an emergency abroad or a personal emergency at home.
As of April 16, 2024, the Public Health Agency of Canada (PHAC) has maintained a Level 2 (Practice Enhanced Health Precautions) travel advisory indicating an increased risk to travelers, or certain groups of travelers including pregnant women, campers, and people visiting friends and relatives. In addition to following the usual health precautions specific to their travel destination, people are reminded to use appropriate personal protective equipment, consider delaying travel until risk is lower, keep up to date on vaccination recommendations and avoid high-risk activities.
On August 30, 2022, the Public Health Agency of Canada (PHAC) updated their travel advisory to state that anyone who becomes symptomatic and/or infected with mpox may be subject to the procedures at their destination, including isolation. There is a risk of limited access to timely and appropriate health care while abroad and delays in returning home.
As reported on June 27, 2022, the World Health Organization (WHO) does not recommend adopting any measures restricting international traffic for either incoming or outgoing travelers. They advise anyone who is symptomatic, suspected, or confirmed case to avoid non-essential travel. Anyone who becomes symptomatic upon returning from travel or while travelling should report to a health professional providing all recent travel information, immunization history and information about close contacts. Public health officials will need to work with travel operators and public health to perform appropriate contact tracing and case investigation.
PHAC: Travel Advisory Level 2 (July 15, 2022)
PHAC: Updated Travel Advisory (Aug 30, 2022)
Government of Canada: Registration for Canadians Abroad
WHO: Travel Advice (June 27, 2022)
What measures should be taken for a suspected mpox case or contact?
Canadians should be made aware of the symptoms of mpox and are advised to report any concerns to their health care provider without delay. The Public Health Agency of Canada has sent alerts to public health authorities to assist health care providers to identify patients showing signs or symptoms consistent with mpox, regardless of any reported travel or any specific risk factors.
Airborne, droplet, and contact precautions are recommended in a healthcare setting. Health care providers should ensure patients with suspected cases of mpox isolate from other family members and pets and should only leave home to seek medical care. The receiving healthcare setting should be notified prior to the patient’s arrival, and patients with suspected, probable, or confirmed mpox infection should not use public transportation. Lesions should be covered with long sleeves and pants, and surgical masks should be worn by the patient and all family members in the household. Surgical gloves should be worn when in direct contact with lesions and disposed of immediately in accordance with the local health regulations. The Public Health Agency of Canada recommends consulting the Interim guidance on infection prevention and control for suspect, probable or confirmed mpox within healthcare settings for more information.
Government of Canada: mpox – For health professionals – Infection prevention and control guidelines